Five Compelling Reasons to Use G.E.D
Glycemic Endothelial Drink (G.E.D.) is a must-use protocol for most surgical patients within an enhanced recovery program. G.E.D. offers distinct benefits and advantages relative to other carb-loading beverages, sports drinks, and fruit juices, which can worsen perioperative hyperglycemia and increase the risk of mortality and morbidity. G.E.D. delivers fluid and electrolytes, maltodextrin as a complex carbohydrate, chromium, and L-Citrulline to support insulin sensitivity and Arg/ADMA ratios in the preoperative period. G.E.D.’s revolutionary formula and protocol are supported by dozens of recently published scientific papers.
1. Postoperative hyperglycemia occurs extremely frequently after major surgeries, and is associated with increased risk of mortality and morbidity.
- Postoperative hyperglycemia (high blood glucose) is related to undiagnosed insulin resistance due to the surgical stress response. It occurs extremely frequently after major surgical procedures:
- 40% of patients experience a postoperative blood glucose >140 mg/dL
- 25% of patients can develop levels of >180 mg/dL.
- Stress-induced insulin resistance is frequently not monitored and therefore may be treated only in <50% of hyperglycemic patients.
- The SCOAP group revealed an almost 30% rate of hyperglycemia with a 2-fold increase in infection, a 1.8-fold increase in reoperation, and a 2.7-fold increase in mortality.
- Aggressive treatment of hyperglycemia, although capable of reducing surgical complications, can be associated with hypoglycemia-related complications and an increased cost of care.
SUPPORTING RESEARCH
- Levetan CS, Passaro M, Jablonski K, et al. Unrecognized diabetes among hospitalized patients. Diabetes Care. 1998;21:246–249.
- Frisch A, Chandra P, Smiley D, et al. Prevalence and clinical outcome of hyperglycemia in the perioperative period in noncardiac surgery. Diabetes Care. 2011;33:1783–1788.
- McConnell YJ, Johnson PM, Porter GA. Surgical site infections following colorectal surgery in patients with diabetes: association with postoperative hyperglycemia. J Gastrointest Surg. 2009;13:508–515.
- Ambiru S, Kato A, Kimura F, et al. Poor postoperative blood glucose control increases surgical site infections after surgery for hepatobiliary-pancreatic cancer: a prospective study in a high-volume institute in Japan. J Hosp Infect. 2008;68:230–233.
- Kotagal M, Symons RG, Hirsch IB, Umpierrez GE, Dellinger EP, Farrokhi ET, Flum DR; SCOAP-CERTAIN Collaborative. Perioperative hyperglycemia and risk of adverse events among patients with and without diabetes. Ann Surg. 2015 Jan;261(1):97-103.NICE-SUGAR Study Investigators, Finfer S, Chittock DR, Su SY, Blair D, Foster.
- D, Dhingra V, Bellomo R, Cook D, Dodek P, Henderson WR, Hébert PC, Heritier S, Heyland DK, McArthur C, McDonald E, Mitchell I, Myburgh JA, Norton R, Potter J, Robinson BG, Ronco JJ. Intensive versus conventional glucose control in critically ill patients. N Engl J Med. 2009 Mar 26;360(13):1283-97.
- Brunkhorst FM, Engel C, Bloos F, Meier-Hellmann A, Ragaller M, Weiler N, Moerer O, Gruendling M, Oppert M, Grond S, Olthoff D, Jaschinski U, John S, Rossaint R, Welte T, Schaefer M, Kern P, Kuhnt E, Kiehntopf M, Hartog C, Natanson C, Loeffler M, Reinhart K; German Competence Network Sepsis (SepNet). Intensive insulin therapy and pentastarch resuscitation in severe sepsis. N Engl J Med. 2008 Jan 10;358(2):125-39.
2. “Carbohydrate loading” offers perioperative benefits.
- Two earlier trials (Soop J et al) demonstrated a potential role for carbohydrate loading in reducing postoperative insulin resistance and the resulting hyperglycemia.
- Although data demonstrates the safety of preoperative consumption of 50 gram maltodextrin drinks prior to surgery, the PROCY study failed to demontrate a true reduction in glycemic variability (number of episodes per day) nor a reduction in complication rates compared to water.
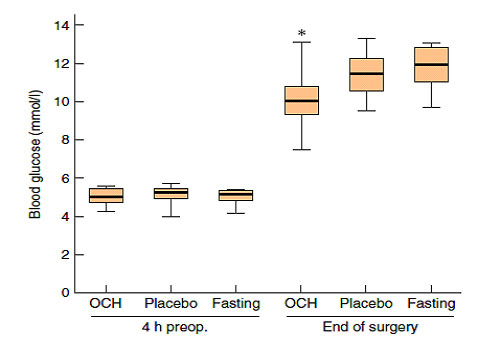
- E.D. has demonstrated consistent significant reductions in glycemic variability using the 25 gram maltodextrin/3 gram citrulline preparation in 3 separate doses preoperatively for colectomy and bariatric surgery compared to sports drinks or grape juice.
SUPPORTING RESEARCH
- Soop M, Nygren J, Myrenfors P, Thorell A, Ljuungqvist O. Preoperative oral carbohydrate treatment attenuates immediate postoperative insulin resistance. Am J Physiol Endocrinol Metab. 2001;280: E576–E583.
- Soop M, Nygren J, Thorell A, Weidenhielm L, Lundberg M, Hammarqvist F, Ljungqvist O. Preoperative oral carbohydrate treatment attenuates endogenous glucose release 3 days after surgery. Clinical Nutrition. 2004;23, 733–7.
- Bilku DK, Dennison AR, Hall TC, Metcalfe MS, Garcea G. Role of preoperative carbohydrate loading: a systematic review. Ann R Coll Surg Engl. 2014;96: 15–22.
- Gianotti L, Biffi R, Sandini M, Marrelli D, Vignali A, Caccialanza R, ViganòJ, Sabbatini A, Di Mare G, Alessiani M, Antomarchi F, Valsecchi MG, BernasconiDP. Preoperative Oral Carbohydrate Load Versus Placebo in Major ElectiveAbdominal Surgery (PROCY): A Randomized, Placebo-controlled, Multicenter, PhaseIII Trial. Ann Surg. 2018 Apr;267(4):623-630.
- Kielhorn BA, Senagore AJ, Asgeirsson T. The benefits of a low dose complexcarbohydrate/citrulline electrolyte solution for preoperative carbohydrateloading: Focus on glycemic variability. Am J Surg. 2018 Mar;215(3):373-376.
- Knight P, Chou J, Dusseljee M, Verseman S, Elian A. Effective reduction instress induced postoperative hyperglycemia in bariatric surgery by better carbloading. Am J Surg. 2019 Nov 9.
3. “Carb loading” with sports drinks or higher-glycemic index maltodextrin drinks does not solve, and can worsen, the problem of postoperative hyperglycemia.
- The recently published PROCY study demonstrated that the commonly recommended higher doses of carbohydrates prior to surgery were associated with a 25% rate of hyperglcemia which did not reduce the risk of SSI.
- Sports drinks contain simple sugars, and therefore were NOT designed to avoid hyperglycemia in insulin-resistant states.
- Even high doses of maltodextrin (40-50 grams) are capable of producing elevated glucose levels (see below; mmols x 18= mg/dl)
Wang, et al. British Journal of Surgery. 2010;97: 317–327.
- G.E.D. uses maltodextrin as the sole source of carbohydrate; the maltodextrin level is low enough to minimize the risk of a spike in glucose postoperatively, while still providing insulin sensitixation.
See Research: Benefits of G.E.D. versus other Options for “Carb Loading”
SUPPORTING RESEARCH
- Wang ZG, Wang Q, Wang WJ, Qin HL. Randomized clinical trial to compare the effects of preoperative oral carbohydrate versus placebo on insulin resistance after colorectal surgery. British Journal of Surgery. 2010;97: 317–327.
4. Reduced Arg/ADMA ratio due to surgical stress is associated with higher risk for adverse events postoperatively.
- Surgical stress reduces serum L-Citrulline and arginine, while also increasing serum ADMA, defined as a reduced Arg/ADMA ratio defined as a 20-25% reduction in the Arg/ADMA ratio perioperatively. This reduction is clearly related to reduced endothelial dysfunction.
- The Arg/ADMA ratio defines systemic arginine bioavailability for endothelial function, immune function, and wound healing.
- Elevation of ADMA has been identified as an independent risk factor for future adverse cardiovascular events and death
- Elevation of ADMA ranked as the first and strongest predictor for outcome in critically ill patients in the intensive care unit.
- Elevated plasma ADMA concentrations are independently associated with a higher risk for adverse events in the peri and postoperative periods.
SUPPORTING RESEARCH
- Luca Gianotti, MD, ScD, Roberto Biffi, MD, Marta Sandini, MD, Daniele Marrelli, MD, Andrea Vignali, MD, Riccardo Caccialanza, MD, Jacopo Vigano, MD, Annarita Sabbatini, RD, Giulio Di Mare, MD, Mario Alessiani, MD, Francesco Antomarchi, MD, Maria Grazia Valsecchi, PhD, and Davide P. Bernasconi, PhD. Preoperative Oral Carbohydrate Load Versus Placebo in Major Elective Abdominal Surgery (PROCY). Annuals of Surgery 2017.
- Neli Ragina, Gabrielle Davis, Michael Doorly , Kyle Cologne, Anthony J. Senagore: Arginine/Asymmetric Dimethylarginine Ratio in Colorectal Surgery. Elmer Press J Clin Med Res. 2017;9(7):555-559
- Valkonen VP, Paiva H, Salonen JT, et al: Risk of acute coronary events and serum concentration of asymmetric dimethylarginine. Lancet .2001;358:2127–2128.
- Boccali C, Bode-Böger S, Mallamaci F, et al: Plasma concentration of asymmetric dimethylarginine and mortality in patients with end-stage renal disease: A prospective study. Lancet. 2001;358:2113–2117.
- Lu TM, Ding YA, Lin SJ, et al: Plasma levels of asymmetric dimethylarginine and adverse cardiovascular events after percutaneous coronary intervention. Eur Heart. J 2003;24: 1912–1919.
- Nijveldt RJ, Teerlink T, Van Der Hoven B, et al: Asymmetric dimethylarginine (ADMA) in critically ill patients: high plasma ADMA concentration is an independent risk factor of ICU mortality. Clin Nutr. 2003;22:23–30.
- Lewin I, Lerner AG, Green SH, et al: Physical Maas R, Dentz L, Schwedhelm E, Thoms W, Kuss O, Hiltmeyer N, Haddad M, Klöss T, Standl T, Böger RH. Elevated plasma concentrations of the endogenous nitric oxide synthase inhibitor asymmetric dimethylarginine predict adverse events in patients undergoing noncardiac surgery. Crit Care Med 2007;35:1876–1881.
5. L-Citrulline supplementation offers advantages for the surgical patient.
- L-Citrulline supplementation has demonstrated an ability to maintain serum levels of arginine better than arginine and without the GI side effects of oral arginine, supporting Arg/ADMA ratios.
- L-Citrulline also reduces insulin resistance by phosphorylation of protein Kinase B (Akt) and inhibiting liver Gluconeogenesis.
SUPPORTING RESEARCH
- Schwedhelm E, Maas R, Freese R, Jung D, Lukacs Z, Jambrecina A, Spickler W, Schulze F, Böger RH. Pharmacokinetic and pharmacodynamic properties of oral L-citrulline and L-arginine: impact on nitric oxide metabolism. Br J Clin Pharmacol. 65:1, 51–59.
- H, Momoo M, Ma X, Huang Y, Suguro S, Yamagishi Y, Gao M. L-Citrulline increases hepatic sensitivity to insulin by reducing the phosphorylation of serine 1101 in insulin receptor substrate-1. BMC Complement Altern Med. 2015 Jun 18;15:188.